Protecting The Kidneys When Receiving Vancomycin
Category: Legal Nurse
Author: Georgina Tyburski
Posted:
May 8, 2015
Kidneys serve the body as a natural filter of the blood and remove water soluble wastes which are directed to the bladder. They play a very essential regulatory role in the urinary system and also serve homeostatic functions such as regulation of electrolytes, maintenance of acid-base, and regulation of blood pressure.
A 74 year old female (named Mattie for the purpose of this article) was admitted to the hospital for treatment for a chronic infection of the right lower leg with osteomyelitis a concern. Mattie's past medical history is complicated with cirrhosis of the liver, deep vein thrombosis, and obesity. Her wound cultures are positive for staphylococuss aureus a gram-positive organism. The doctor orders a glycopeptide antibiotic commonly known as vancomycin to be administered. Mattie is to receive vancomycin 15mg/kg intravenously every 12 hours. During Mattie's hospital course she is cleared by cardiology, hematology, and infectious disease to have surgical intervention in hopes of improving the chronic lower leg infection. Following surgery she experiences nausea with little to no oral intake for several days. Intravenous replacement was initiated.
Mattie's worsening condition is noted with generalized edema, brown urine and little output despite continued fluid boluses and the administration of lasix. Lab results showed evidence of acute renal failure resulting in a nephrology consult.
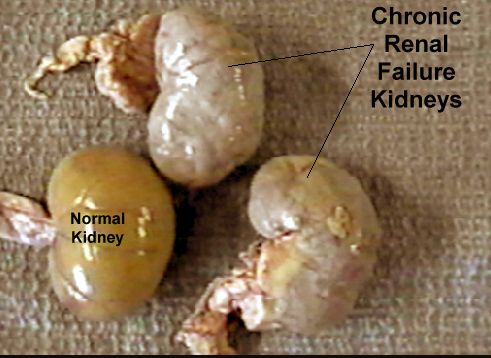 Mattie is diagnosed with acute renal failure resulting from hepatorenal syndrome (a life threatening condition that consists of rapid deterioration in kidney function in individuals with liver cirrhosis or liver failure usually fatal unless liver transplant performed), and acute tubular necrosis (death of epithelial cells that form renal tubules of kidneys). With no prior history of renal disease, Mattie's kidneys have undergone cellular death and are unable to filter wastes, produce urine and maintain fluid balances. This dysfunction has caused a build up of toxins in her body affecting the blood, brain and heart, as well as other complications. Mattie's kidney failure is very serious and even deadly if left untreated. The treatment at this point will include dialysis only if she is able to tolerate such an invasive procedure without progressing to life-threatening events, including death.
Mattie is diagnosed with acute renal failure resulting from hepatorenal syndrome (a life threatening condition that consists of rapid deterioration in kidney function in individuals with liver cirrhosis or liver failure usually fatal unless liver transplant performed), and acute tubular necrosis (death of epithelial cells that form renal tubules of kidneys). With no prior history of renal disease, Mattie's kidneys have undergone cellular death and are unable to filter wastes, produce urine and maintain fluid balances. This dysfunction has caused a build up of toxins in her body affecting the blood, brain and heart, as well as other complications. Mattie's kidney failure is very serious and even deadly if left untreated. The treatment at this point will include dialysis only if she is able to tolerate such an invasive procedure without progressing to life-threatening events, including death.
This scenario is often a risk when patients receive vancomycin. It is a very delicate process to ensure that the patient receives the most appropriate and effective dose without causing damage to the kidneys. Vancomycin is used in the treatment of serious staphylococci, streptococci, and other gram-positive organisms. It is the drug of choice for infections due to methicillin-resistant staphylococci also known as MRSA. Nephrotoxicity can occur after excessive doses of these agents. The administration of vancomycin requires close monitoring of labs including the BUN, creatinine and trough levels to ensure the patient is receiving the therapeutic does without causing damage to their kidneys.
BUN: Blood urea nitrogen is a lab test monitoring nitrogen in the blood in the form of urea, the metabolic product of the breakdown of amino acids used for energy production. The normal concentration is 8 to 18mg/dl. The level of urea in the blood provides a rough estimate of kidney function with elevation levels seen in the presence of dehydration, decreased renal function, upper gastrointestinal bleeding or treatment with drugs such as steroids or tetracycline's.
Creatinine: The decomposition product of the metabolism of phosphocreatine, a source of energy for muscle contraction. Increased quantities of it are found in advanced stages of renal disease. The average normal serum creatinine value is less then 1.2 mg/dl. Vancomycin monitoring also consists of obtaining trough levels. It is still recommended for patients receiving doses of vancomycin every 24 hours, trough levels should be drawn 30 minutes prior to the 4th dose. If the patient has severe renal failure a trough may be checked prior to the 2nd dose; however, this level is NOT at steady state and will go up with subsequent doses.
Goal trough: 10-20mcg/ml, vancomycin troughs <10mcg/ml may lead to resistance. Some serious infections may require higher trough levels of 15-20 mcg/ml., serious infections, including:
-
Pneumonia
-
Endocarditis
-
Meningitis
-
Osteomyelitis
-
Bacteremia
-
Sepsis/Septic shock
-
Known MRSA infection
Key points for adjustments: 1) make sure the trough level was drawn appropriately and all previous doses were given. 2) Be aware of changing renal function. Today's level is reflective of how the patient cleared the vancomycin in the past 24-48 hours and may not reflect how it will be cleared tomorrow. If renal function is improving or impaired, this should be considered in the adjustments of dosing. 3) If high levels require holding a dose then it is recommended do not restart the same regimen. This indicates the patient cannot clear this much vancomycin. High levels require a dosage/interval adjustment. 4) Adjusting vancomycin doses is mostly trial and error and close monitoring of patient response is necessary to ensure appropriate treatment. It is very important to account for changing in renal function in all patient's receiving vancomycin. Monitoring can include repeated lab work such as BUN and Creatinine. Signs and symptoms of kidney failure include: little or no urine (oliguria), swelling in the legs and feet, loss of appetite, nausea and vomiting, confusion, anxiety, restlessness, weakness, shortness of breath and lethargy. It is imperative that patients receive a thorough assessment observing for signs and symptoms of kidney failure as well as close monitoring of intake--oral and intravenous fluids and urine output.
There is Stroke Alert, Code STEMI, Code rescue and Code blue just to name a few of the acronyms to alert health care workers that time is critical to preserve patients lives when organs are at risk for failure. The kidneys stand alone in this vocabulary. The only alert button for kidney failure prevention is the health care team to be alert to warning signs and symptoms of progressing kidney failure from toxins.
In Mattie's case she was a mishap of poorly managed vancomycin therapeutic dose monitoring. Her kidneys were poorly protected when receiving vancomycin.
Is your client a victim of poorly managed vancomycin dose monitoring?
Do you know the warning signs and symptoms of progressing kidney failure from toxins?
Our EXPERTS are chosen for their outstanding knowledge and experience in their area of specialty,
and can analyze your case for overlooked symptoms of kidney failure.
